Human Influenza
Background: Influenza virus causes respiratory infections (“the flu”) that can be quite severe. About 36,000 people die from flu complications every year in the U.S. The symptoms of the flu include fever, headache, sore throat, cough, and muscle aches. These symptoms are difficult to distinguish from other respiratory infections. A more definitive diagnosis can be made by testing respiratory fluids, often obtained via a throat or nasopharyngeal swab, for the presence of influenza proteins (using ELISA or similar techniques) or nucleic acid (using RT-PCR) (Since the virus genetic material is RNA, reverse transcription (RT) is used to copy the RNA into cDNA for the PCR test). Since it takes a few weeks for antibodies to influenza to be detected in a patient’s blood, testing the patient’s blood for influenza antibodies is usually used to confirm an infection after the illness has subsided, e.g. to monitor the extent of an epidemic. Influenza virus is highly contagious and is easily spread via respiratory droplets. There are drugs available to treat influenza virus infections, but they are generally only used when an infected person is at risk for serious complications, or to control an epidemic. The influenza vaccine (“flu shot”) can protect individuals from getting infected, and it is highly recommended for individuals most at risk for the serious complications from flu, such as people older than 65, children under 2 years old, and anyone with chronic heart or lung conditions. The vaccine usually contains three different strains of influenza, and the antibodies generated to the vaccine can protect against these strains and related strains. Influenza virus has a high mutation rate and there are new strains of the virus appearing every year. There are two main strains of influenza, A and B, that cause the annual outbreaks of flu. Strain A viruses are further distinguished based on their surface proteins, abbreviated H and N. The strain names also include the location and year where they were isolate. For example, strain A/Fujian/02 (H3N2) was isolated in the Fujian province in China in 2002 and its surface proteins are designated H3N2.
Case A. This fall, for the first time in several years, Sheila did not get a flu shot. She has been very busy, especially since she started babysitting her grandchildren (ages 1 and 3) on weekdays. She also does not like needles and shots, so it was easy for her to come up with excuses not to go get the shot. Sheila is 67 years old, but she has been in good health and does not have any chronic health conditions. Two days ago, she came down with a fever (102 degrees F), sore throat, and a bad cough. She has been taking ibuprofen, but it does not seem to be helping. Sheila feels just awful, but she drags herself to the clinic. The physician is concerned that the fever has not subsided, and because Sheila’s age places her at some risk for serious complications from influenza, she decides to test Sheila for influenza and takes a throat swab sample. Although Sheila’s grandchildren have not been with her the past two days, they did stay at her house the day before she got sick. The physician suggests that both children be tested, even though they have not yet shown any symptoms.
To analyze this case, first run an ELISA on the throat swab samples from the following sources to test for the presence of influenza virus proteins, using antibodies specific for influenza A and B viruses. Then perform a PCR test on the cDNA isolated from the swabs, using primers specific for influenza A and B, to see if influenza virus genetic material can be detected.
Protein and DNA samples:
Negative control (no influenza virus)
Positive control for influenza A
Positive control for influenza B
Sheila
1-year old grandchild
3-year old grandchild
Run the ELISA
Run the PCR test
Questions:
- Do Sheila’s symptoms appear to be caused by infection with influenza virus?
- Are either of the grandchildren infected?
- What should the physician recommend for treatment for these patients?
- What should Sheila do to avoid spreading her illness to others?
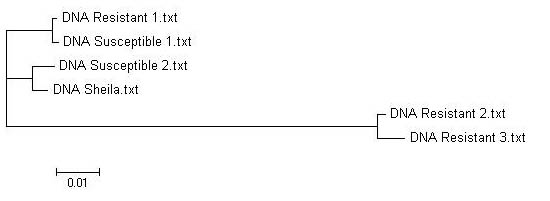
Sequence analysis: Influenza B viruses generally respond well to the antiviral drugs oseltamivir (Tamiflu) and zanamivir (Relenza), which inhibit neuraminidase activity. However, influenza B viruses have been isolated this season that show some resistance to oseltamivir. Compare the neuraminidase sequence isolated from Sheila’s virus to these resistant virus isolates as well as to some drug-sensitive viruses. Does it look like oseltamivir will be an effective treatment for Sheila? What other options does she have?
{kind=link}