HIV/AIDS
Background: Human immunodeficiency virus (HIV) causes the disease Acquired Immunodeficiency Syndrome (AIDS). AIDS is characterized by the inability to mount an effective immune response to bacteria and other pathogens, resulting in a variety of life-threatening infections. The virus is spread when bodily fluids, such as blood and semen, from an infected person directly enter the bloodstream or tissue fluids of an uninfected person. For example, unprotected sexual intercourse and sharing needles during injected drug use can spread the virus. Once in the body, HIV infects and destroys certain white blood cells (called CD4 cells) and impairs the immune system. It may take years after the initial HIV infection for the symptoms of AIDS to appear. HIV infection is routinely detected indirectly, via tests which measure whether a person’s blood contains antibodies against HIV; if so, they must have been previously infected with the virus. Recently, a viral load test was developed which directly measures the amount of HIV in a person’s blood or lymph nodes using the PCR technique. For additional information about HIV/AIDS-related disease, detection methods, treatment, and prevention, visit the CDC’s web site, www.cdc.gov/hiv .
These case scenarios are based on real people infected with HIV. Each case includes a video, accessed from the Case It web site, showing that person discussing their experience with the disease. As you study the cases, here are some general questions you might consider:
- How did this person become infected with HIV?
- Have others also been infected? Who else should be tested?
- How reliable are the tests?
- How often should someone be tested?
- Why do people engage in risky behaviors?
- What impact is the infection having on this person’s life?
- How can this person prevent further transmission of the virus?
- What other ethical decisions does this person face?
- How common is this case?
- Are there cultural differences regarding attitudes about HIV and prevention?
Anna is a 27-year-old women from Guatemala, who is living with her boyfriend and is pregnant with her first child. A blood test during her second trimester revealed that she was HIV positive. Anna is surprised, because her first trimester test was negative, and she did not have sexual contact with anyone other than her boyfriend. She is very concerned about the fate of her child, who may contract the virus from Anna.
Blood samples for ELISA and Western blot:
Anna, first trimester
Anna, second trimester
Anna’s baby, 6 weeks after birth
Anna’s boyfriend
Positive and negative controls
Run an ELISA to test blood samples for the presence of antibodies to HIV. The ELISA involves adding antibody samples to wells of a 96-well plate that have been coated with HIV proteins. Samples produce color in the wells if they contain antibodies that can bind to the HIV proteins. An ELISA test is generally considered positive if the color production (absorbance) for a sample is at least twice that of the negative control, thought this would be determined empirically for each run.
Run the ELISA
Since the ELISA has a 1/1000 rate of false positive results, positive ELISA results are confirmed by Western blot. For the Western blot, HIV proteins are separated by size using polyacrylamide gel electrophoresis. Then blood samples are tested to see whether they bind specific proteins in the gel. The HIV proteins visible in the gel (from largest to smallest, running left to right), include gp160*, gp120, p55, p41, p31 and p24. The positive control antibody will bind to all of the proteins. To be considered HIV positive, a sample must bind to two of these three proteins: gp160/gp120*, gp41, and p24. Any other binding pattern is considered “indeterminate”. A result can only be called negative if there is no binding to any of the HIV proteins. (*gp160 is a precursor that includes both gp120 and gp41, before they are cleaved into separate envelope proteins; antibodies that bind gp120 are likely to also bind gp160.)
Run the Western blot
Questions:
- What is the status of each person tested? How would you explain these results to Anna?
- How would explain the difference between Anna’s first and second trimester results?
- What recommendations would you give Anna as she cares for herself and her baby
- How did Anna get infected? How did her partner get infected?
- Why did Anna think it was OK to have unprotected sex with her partner?
- What does an indeterminate test mean for the baby? Should the baby be tested again?
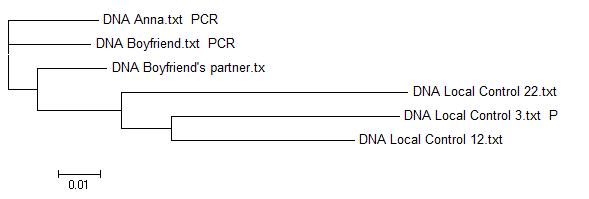
Sequence analysis: Did Anna’s partner infect her with HIV? Compare Anna’s and her boyfriend’s HIV sequence with local controls – does tree suggest that their sequences are more similar than random samples? Can you tell from this who gave it to whom? Anna’s boyfriend acknowledges that he had another sexual partner. Does adding this sequence help you determine the sources of Anna’s infection?
{kind=link}